Study population
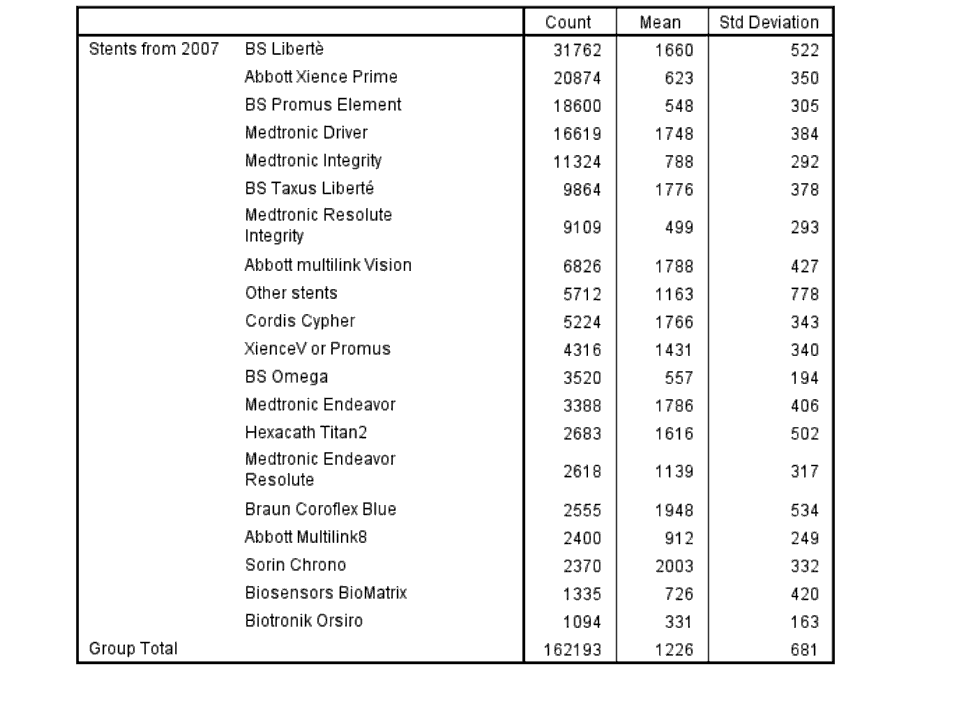
These presentations include all stents used in Sweden from 2007 until the end of enrolment which is shown at the different figures. Stents implanted until the end of 2007 at one small center (Skövde Hospital) were excluded, as this hospital was not recording their subsequent coronary angiographies in SCAAR during this period. Also stents with missing data (less than 1%) were excluded.
The SCAAR registry (SWEDHEART registry)
SCAAR/SWEDHEART records consecutive patients from all centres (n=29) performing coronary angiography and PCI in Sweden. The treating physician reports each procedure on-line via a web-interface directly from the catheterization laboratory. In early 2004 an interactive method for registration of restenosis was implemented in SCAAR. During the registration of a coronary angiography or PCI a mandatory question regarding the existence of any type of restenosis has to be answered. A detailed interactive presentation of all previously (in Sweden) treated coronary segments of the patient is displayed. Information about date, hospital and coronary segment together with name and dimension of stents used are shown. The treating physician must record any restenosis and, from April 2005, also information about acute occlusions in the specified stents. From 2007 also non-occlusive angiographical stent thrombosis is reported in SCAAR.
Definitions
In the SCAAR registry, if a patient undergoes repeat coronary angiography or PCI for any indication, operators are informed by the system about the characteristics of the previous procedure(s) and treated lesions, if any. For each previously treated lesion, the operator should fill in if restenosis or stent thrombosis has occured. Restenosis, as registered in SCAAR, is defined as a stenosis assessed by angiographic visual estimation (>50%) and/or as judged by another invasive method (as FFR, IFR, IVUS or OCT) in a previously implanted stent identified by coronary angiography for any clinical indication performed anywhere in the country. In keeping with the Academic Research Consortium, definite stent thrombosis is defined as symptoms suggestive of an acute coronary syndrome and angiographic evidence of stent thrombosis. In the SCAAR registry, if a patient undergoes repeat coronary angiography or PCI for any indication, operators are informed by the system about the characteristics of the previous procedure(s) and treated lesions, if any. For each previously treated lesion, the operator should fill in if restenosis or stent thrombosis has occured.
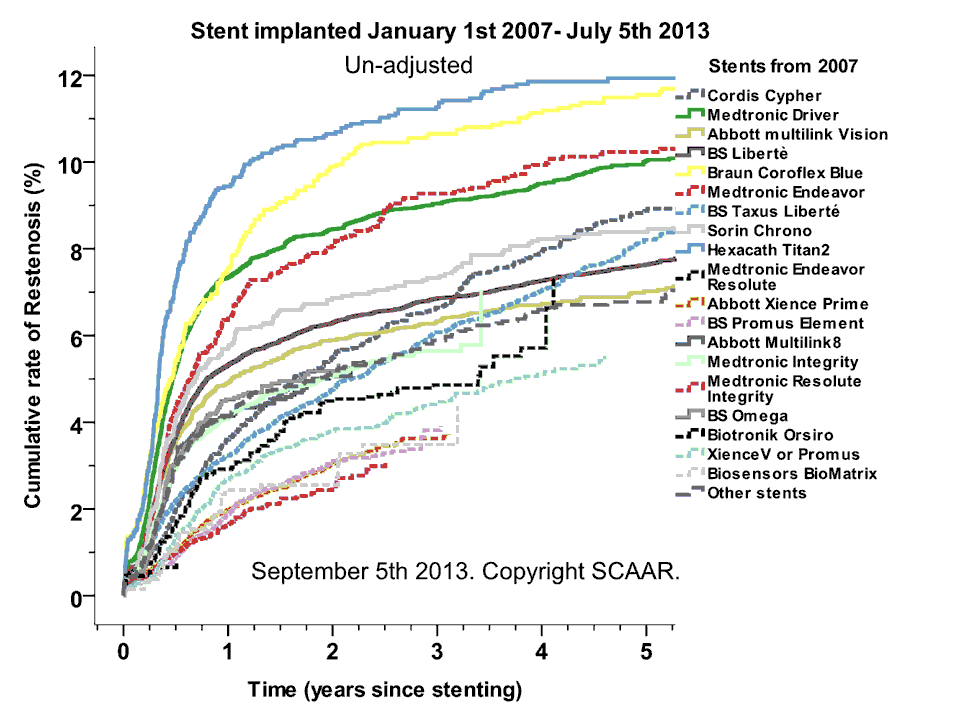
Restenosis, as registered in SCAAR, is defined as a stenosis assessed by angiographic visual estimation (>50%) or by fractional flow reserve FFR ≤ 0.80 in a previously stented segment identified by coronary angiography for any clinical indication performed anywhere in the country.
Stent thrombosis is defined as symptoms suggestive of an acute coronary syndrome and angiographic evidence of stent thrombosis.
TLR (Target Lesion Revscularizations) is defined as a new treatment of the same coronary segment in a new PCI.
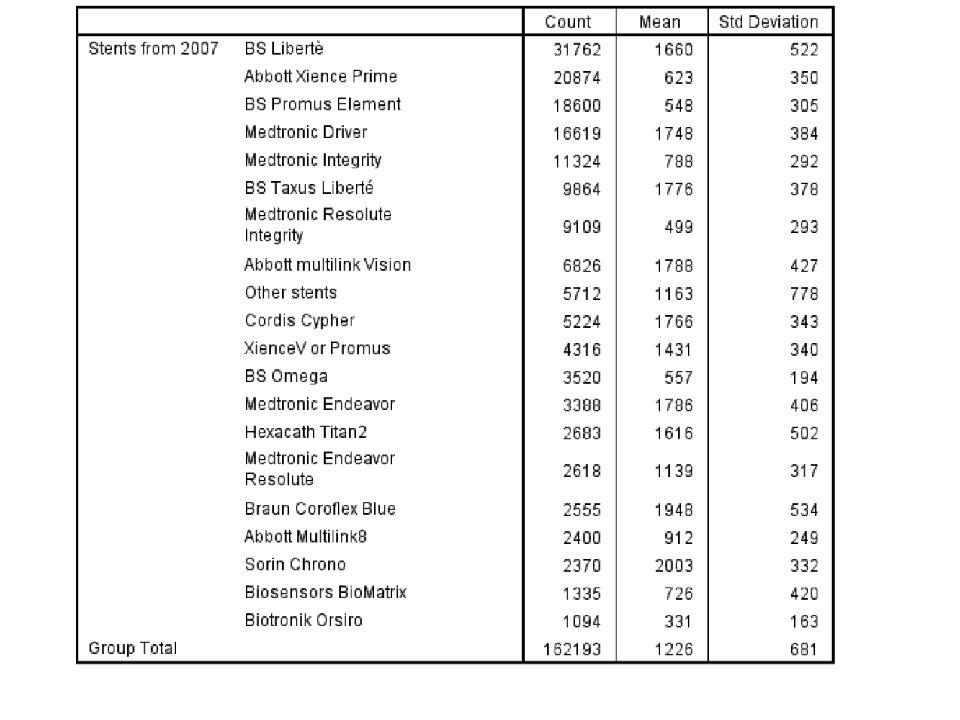
Stents implanted at more than 1000 occasions in Sweden during the study period are separately analyzed and presented. However if specified also stents used less often may be presented.
The names of the different stents are presented as they are entered in the database. Some similar stents are analysed together. The Multi-Link Vision® and the Multi-Link MiniVision® (Abbot Laboratories, USA) are both referred to as “Abbott multilink Vision”; Medtronic Driver® coronary stent and Medtronic Micro-Driver® coronary stent (Medrtonic Inc, USA) as “Medtronic Driver”; Cordis Cypher® and Cypher Select® (Cordis Corporation, USA) as “Cordis Cypher”; The Abbott XienceV and the Boston Scentific Promus stent are reported as “Xience V Promus”.
Statistical analyses
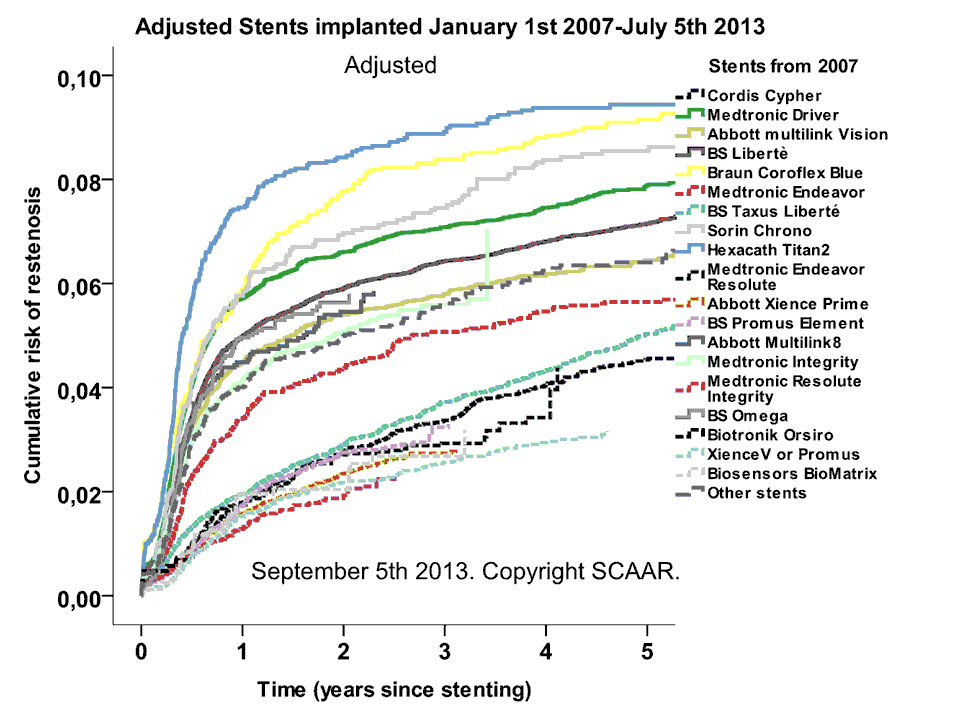
Cumulative event rates are estimated by the Kaplan-Meier method. The primary endpoint is the registration of stent thrombosis or restenosis in SCAAR.
All calculations are performed with a focus on individual stents. Thus the data are presented from the stent perspective with patient and procedure data linked to the individual stents.
In the analysis August 17th 2009 0,8 % of the stents were excluded from the analysis due to missing data. However, this group had a very similar rate of acute stent occlusions compared to those with complete data; RR (95% Confidence Interval), 0.998 (0.536-1.860).
The present study is exclusively descriptive and should only be regarded as hypothesis generating.
Copyright: ©SCAAR/SWEDHEART owns the rights of the presentations, but the pictures can freely be used with the reference of origin.
This web-site presents information about clinical and angiographical results of coronary stenting with different types of stents. Updates will be posted regularly reportin angiographically verified stent occlusions with an acute clinical presentation. This event is the SCAAR substitute for the ARC definition of “definite stent thrombosis”. The difference is that non-occlusive stent thromboses are not registered in SCAAR during the whole follow-up time.
Since 2004/2005 (see methodological remarks) each individual coronary stent used in Sweden can be follow regarding important clinical/angiographically endpoints as restenosis and acute occlusions. Our intent with these presentations is not to conclude that any particular stent is “better” or “worse” than any of the other stents. Still we think that it is important to show the un-commented result and thereby maybe by this encourage the performance of prospective randomized studies with direct comparisons between different stents.
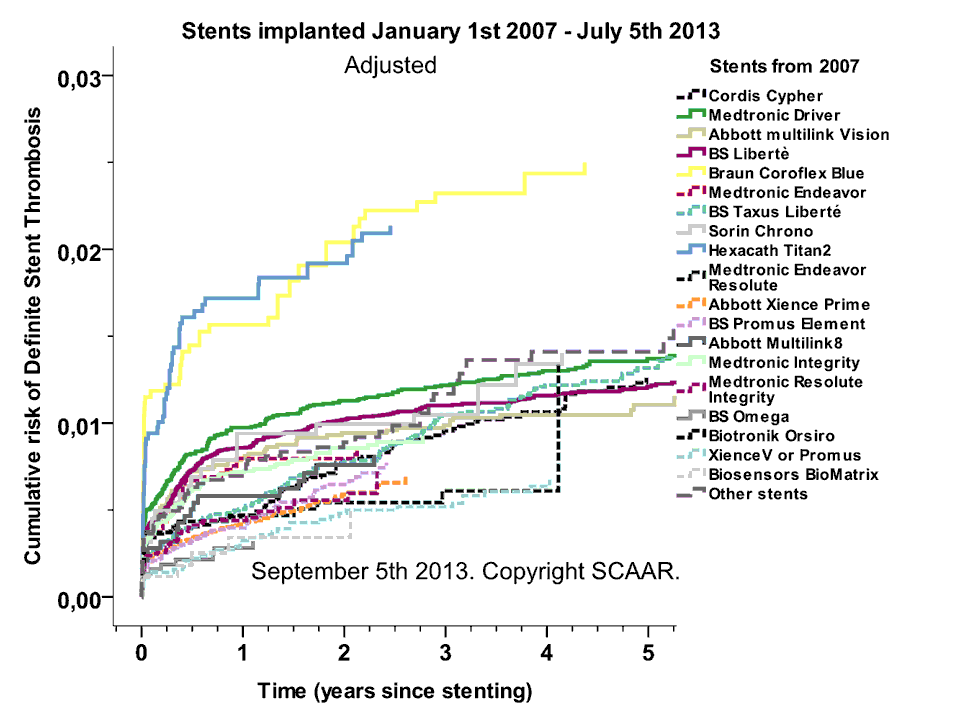
There are many possible factors that may influence the results of stenting with different stents. We have tried to compensate for some of these by introducing all available different background , clinical and procedural factors registered in our registry in a multivariable statistical model (see methodological remarks), However, some factors of known importance both for the selection of stent type and the result, such as bail-out stenting in complex situations, large coronary dissections and stenting in specific types of complex vessels (tourtous and or calcified), are not registered in our registry. The best way to compare the performance and outcome is by randomized trial.
(January 19th 2012): Since beginning of 2007 is in not only possible to analyse acute stent occlusions in the database but also occurance of non-occlusive angiographical thrombus. Acute stent occlusion or non-occlusive thrombus in a previously inplanted stent (with acute clinical presentation) are now presented as Stent Thrombus for stents inplanted since 2007. Presentation of reported restenosis are also added since 2007 for stents used i Sweden at least 1000 times.
Presentations:
Angiographically verified stent occlusions with acute clinical presentation (Stent thrombosis):







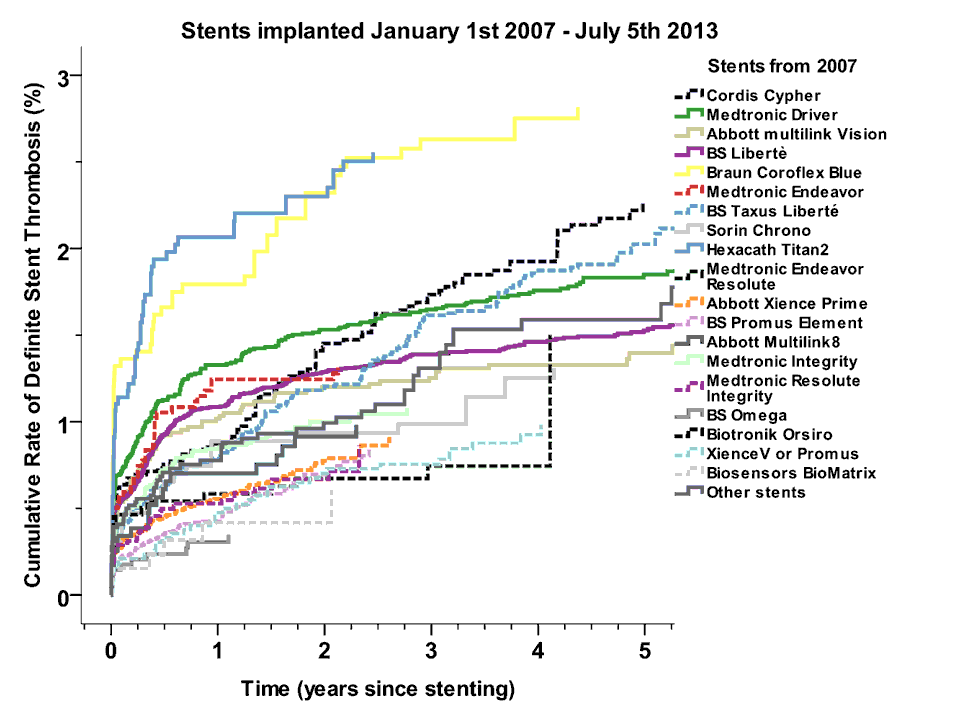

This web-site presents information about clinical and angiographical results of coronary stenting with different types of stents. Updates will be posted regularly reporting angiographically verified stent thrombosis with an acute clinical presentation. This event is the SCAAR substitute for the ARC definition of “definite stent thrombosis”.
Since 2004/2005 (see methodological remarks) each individual coronary stent used in Sweden can be follow regarding important clinical/angiographically endpoints as restenosis and acute occlusions. Our intent with these presentations is not to conclude that any particular stent is “better” or “worse” than any of the other stents. Still we think that it is important to show the un-commented result and thereby maybe by this encourage the performance of prospective randomized studies with direct comparisons between different stents.
There are many possible factors that may influence the results of stenting with different stents. We have tried to compensate for some of these by introducing all available different background , clinical and procedural factors registered in our registry in a multivariable statistical model (see methodological remarks), However, some factors of known importance both for the selection of stent type and the result, such as bail-out stenting in complex situations, large coronary dissections and stenting in specific types of complex vessels (tortuous and or calcified), are not registered in our registry. The best way to compare the performance and outcome is by randomized trial.
(January 19th 2012): Since beginning of 2007 is in not only possible to analyze acute stent occlusions in the database but also occurrence of non-occlusive angiographical thrombus. Acute stent occlusion or non-occlusive thrombus in a previously implanted stent (with acute clinical presentation) are now presented as Stent Thrombus for stents implanted since 2007. Presentation of reported restenosis are also added since 2007 for stents used i Sweden at least 1000 times.
Presentations:
![]()
![]()
![]()
![]()
![]()










![]()